| |
| Erectile Dysfunction |
| |
| ED: Non-Surgical Management (Erectile Dysfunction) |
|
|
Erectile dysfunction (ED) is a medical term that describes the inability to achieve and or maintain an erect penis adequate for sexual function. This condition is one of the most common sexual problems for men and increases with age. It is estimated between 15 to 30 million American men suffer from ED, although not all men are equally distressed by the problem.
Most men have difficulty with erections from time to time, yet in some men, it is a regular and more severe problem. It can cause low self-esteem, performance anxiety, depression and stress. ED may affect the quality of a marriage or intimate relationships. However, there are many safe and effective ED treatments available. |
| |
|
| What happens under normal conditions? |
|
|
Achieving a normal erection is a complex process involving psychological impulses from the brain, adequate levels of the male sex hormone testosterone, a functioning nervous system, and adequate and healthy vascular tissue in the penis.
The simplest way to describe the process of erection is to think of a washing machine. The "on-off" switch (the brain) initiates the process; the wires in the washing machine (the nerves) carry the electrical signal to the pipes (the blood vessels), when an appropriate signal arrives a valve opens to allow water to flow in (the arteries carry blood into the penis) and the drain shuts (the penile veins close). Water flows in and fills the tank (the penis fills with blood and becomes erect) and the wash cycle begins (enjoys sexual activity). At the end of the wash cycle this process reverses, the switch goes to the off position (the brain terminates erection), the valve closes (the arteries markedly decrease blood inflow) and the drain opens draining the wash tank of water (the veins open, blood leaves the penis and erection subsides). |
| |
|
| How do erections occur? |
|
|
When a man is not sexually aroused, his penis is soft, limp or flaccid. During sexual arousal, nerve messages release chemicals that increase blood flow into the penis. The blood flows into two erection chambers made of spongy tissue (the corpus cavernosum) in the penis. The “smooth muscle” in the erection chambers relaxes, which allows blood to enter and remain in the chambers. The pressure of the blood in the chambers makes the penis firm, producing an erection. After a man has an orgasm, the blood flows out of the chambers and the erection subsides.
|
| |
|
| What are the risk factors for ED? |
|
|
• The most common risk factors for ED are:
• age over 50
diabetes
high blood pressure
high cholesterol
smoking
cardiovascular disease
These diseases over a period, can lead to a degeneration of the penile blood vessels, leading to restriction of blood flow through the arteries and to erectile tissue damage, which allows leakage of blood through the veins during erection.
Abnormally low levels of circulating testosterone may cause ED, although low testosterone is found in a minority of men who develop ED. Low levels of sexual desire, lack of energy, mood disturbances, loss of muscle strength and depression can all be symptoms of low testosterone. A simple blood test can determine if the testosterone level is abnormally low. Low levels of testosterone can be replaced by using a number of different delivery systems (e.g., shots, skin patches, gels, sub-dermal implants).
The choices made in life can lead to degeneration of the erectile tissue and the development of ED. Smoking, drug or alcohol abuse, particularly over periods of time, will compromise the blood vessels of the penis. Lack of exercise and a sedentary lifestyle also contribute to the development of ED. Modifying these risk factors may contribute to overall health and in some individuals correct mild ED.
Patients undergoing surgery or radiation therapy for cancer of the prostate, bladder, colon or rectum are at high risk for the development of ED. Drugs used to treat these risk factors listed above may also lead to or worsen ED.
Another cause of ED is peripheral neuropathy in which the nerves leading to the penis fail to send coordinated signals to the penis. Peripheral neuropathy can be caused by diabetes, HIV infection, certain medications and other less common conditions.
|
| |
|
| What causes ED? |
|
|
ED can result from medical, physical or psychological factors. ED may be caused by a combination of factors that could also include medicine, alcohol or drugs. The physical and medical causes of ED include three basic problems:
Not enough blood flows into the penis. Many conditions can reduce blood flow into the penis, examples include heart disease, diabetes and smoking.
The penis cannot store blood during an erection. A man with this problem, called venous leak or cavernosal dysfunction, cannot maintain an erection because blood does not remain trapped in the penis. This condition can occur to any man regardless of age.
Nerve signals from the brain or spinal cord do not reach the penis. Certain diseases, injury or surgery in the pelvic area can damage nerves in the penis.
Sexual activity requires the mind and body to work together. Psychological, emotional or relationship problems can cause or worsen ED; and include but are not limited to:
• Depression
Relationship conflicts
Stress at home or work
Anxiety about sexual performance
Many prescription and over-the-counter medications may have sides effect often causing erection difficulties. Drugs such as marijuana, heroin, cocaine and alcohol can lead to sexual problems.
If your ED is due to a hormonal problem, such as low testosterone or diabetes, you may be referred to an endocrinologist. Your healthcare provider may also refer you to a mental health professional. These specialists treat psychological or emotional causes of ED. Even if your ED is not caused by these factors, it may contribute to them. It may be helpful to get counseling, alone or with your partner, in addition to getting medical therapy for ED.
|
| |
|
| Who gets ED? |
|
|
Studies show about one-half of American men over age 40 have some degree of ED. At one time, health care providers thought that psychological problems, such as stress and anxiety, were the main causes of ED. Recent studies show most ED cases have a physical cause. While ED becomes more common as men age, growing old is not the cause of the problem. Though sexual function may decrease with age, many men enjoy sexual activity well into their senior years.
ED can be an early warning sign of a more serious illness, such as heart disease, high blood pressure or diabetes mellitus. Diagnosing and treating the condition that causes ED can improve your overall well being, as well as help restore your sexual health.
|
| |
|
| How is ED diagnosed? |
|
|
ED is diagnosed by an urologist or another medical professional and for most patients; the diagnosis will require a simple medical history, physical examination and a few routine blood tests.
• Medical History
exam requires health care providers to ask about you, and your ED experience. The doctor will also want to know if you have any other conditions that might affect your ED, such an any endocrine problems or depression. They may ask questions about your sexual history and performance, which may be very personal but necessary to understand the root cause of the problem. The important thing to remember is not to be embarrassed while speaking with your physician and to be very open to allow for the best treatment options for you. Other questions the physician is likely to ask are the following:
Your current sexual function
When you started noticing changes
Any past medical or sexual problems
Surgery or injury to the pelvic area
Current and past medication usage
Lifestyle and personal habits (i.e. smoking, drinking, use of illicit drugs, etc.)
Relationship with current and past partners
Physical Examinations means the doctor will check your overall health and physical condition. They will look for signs of problems with your circulatory, nervous and endocrine system. This includes checking your blood pressure, penis and testicles and you may need to have a rectal exam to check the prostate. These tests are not painful and may provide valuable information about the cause of ED. Most patients do not require extensive testing before beginning treatment.
The choice of testing and treatment depends on the goals of the individual. If erection returns with simple treatment like oral medication and the patient is satisfied, no further diagnosis and treatment are necessary. If the initial treatment response is inadequate or the patient is not satisfied, then further steps may be taken. In general, as more invasive treatment options are chosen, testing may become more complex.
|
| |
|
| What are some non-surgical treatments? |
|
|
• The first line of therapy for uncomplicated ED is use of oral medications known as phosphodiesterase-5 inhibitors (PDE-5):
sildenafil citrate (Viagra®),
vardenafilHCl (Levitra®),
tadalafil (Cialis®)
Men with ED take these pills before beginning sexual activity and the drugs boost the natural signals that are generated during sex, thereby improving and prolonging the erection itself. The medication works by relaxing the muscle cells in the penis allowing for better blood flow and production of a rigid erection. These medications are often effective, and nearly 80% of men show improvement once they begin use. The drugs are effective regardless of race and age. Although studies have shown these medications can be used by heart patients, men taking nitrates should speak with their physician before use to understand the possible drug interactions or affects on their other health conditions.
The side effects of PDE-5 inhibitors are mild and usually transient, decreasing in intensity with continued use. The most common side effects are headache, stuffy nose, flushing and muscle aches. In rare cases, sildenafil can cause temporary blue-green shading of vision. There is no long-term risk and decreases as the amount of the drug in the body decreases. It is important to follow the medications instructions in order to get the best results. Tests have shown 40 percent of men who do not respond to sildenafil will respond when they receive proper instruction on the medications use.
For men who do not respond to oral medications another drug, alprostadil, is approved for use in men with ED. This drug comes in two forms: injections that the patient places directly into the side of the penis and an intraurethral suppository. Success rates in achieving a firm erection useful for sexual intercourse with self-injection can reach 85 percent. Modifying alprostadil to allow intraurethral delivery avoids the need for a shot, but reduces the likelihood of successful treatment. The most common adverse effects of alprostadil use are a burning sensation in the penis and a prolonged erection lasting over four hours, requiring medical intervention to reverse the erection.
For men who cannot or do not wish to use drug therapy, an external vacuum device may be acceptable. This device combines a plastic cylinder or tube that slips over the penis, making a seal with the skin of the body. A pump on the opposite end of the cylinder creates a low-pressure vacuum around the erectile tissue, which results in an erection. To keep the erection once the plastic cylinder is removed a rubber constriction band goes around the base of the penis, which maintains the erection. With proper instruction, 75 percent of men can achieve a functional erection using a vacuum erection device.
Some men who have severe penis tissue degeneration do not respond to any of the treatments listed above. While this is a small number of men, they usually have the most severe forms of ED. Patients most likely to fall into this group are men with advanced diabetes, men who suffered from ED before undergoing surgical or radiation treatment for prostate or bladder cancer and men with deformities of the penis called Peyronie’s disease. For these patients reconstructive prosthetic surgery (placement of a penile prosthesis or "implant") will create an erection, with patient satisfaction rates approaching 90 percent. Surgical prosthetic placement normally can be performed in an outpatient setting or with one night of hospital observation. Possible adverse effects include infection of the prosthesis or mechanical failure of the device.
|
| |
|
| What can be expected after treatment? |
|
|
All of the treatments, with the exception of prosthetic reconstructive surgery, are temporary and meant for use on demand. The treatments compensate for but do not correct the underlying problem in the penis. It is important to follow-up with your doctor and report on the success of the therapy. If your goals are not reached, if your erection is not of sufficient quality or duration and you are still distressed, you should explore the alternatives with your doctor. Because the medications used are not correcting the problems leading to ED, your response over time may not be what it once was. If such should occur again, have a repeat discussion with your physician about the remaining treatment options.
Frequently Asked Questions: |
| |
|
| How do I know my ED is not in my head? |
|
|
We do not know this for sure. It is impossible to prove that there is no psychological component to a man's ED. Many years ago, doctors thought that most men with ED had psychological problems. We now realize that most men have an underlying physical cause and that the cause of ED is often a combination of physical and psychological factors.
If I worry about my ability to get an erection, can I make a bad condition worse?
Nothing happens in the body without the brain; worrying about your ability to get an erection can itself interfere with the process. This condition is called performance anxiety and can be overcome with education and treatment.
|
| |
|
| If I worry about my ability to get an erection, can I make a bad condition worse? |
|
|
Nothing happens in the body without the brain; worrying about your ability to get an erection can itself interfere with the process. This condition is called performance anxiety and can be overcome with education and treatment.
|
| |
|
| Can I combine treatment options? |
|
|
This is often done but because of the risk of prolonged erections with drug therapy, it should only be performed under physician supervision. Ask your doctor for proper instructions.
I was fine until I began taking this new drug, what should I do?
Many drugs can cause ED, but some cannot be changed because the benefits outweigh the adverse effects. If you are certain, a specific drug has caused the problem, discuss the possibility of a medication change with your doctor. If you must remain on the specific medication causing the problem, the treatment options outlined above can still be used in most cases
|
| |
|
| I was fine until I began taking this new drug, what should I do? |
|
|
Many drugs can cause ED, but some cannot be changed because the benefits outweigh the adverse effects. If you are certain, a specific drug has caused the problem, discuss the possibility of a medication change with your doctor. If you must remain on the specific medication causing the problem, the treatment options outlined above can still be used in most cases
|
| |
|
| |
| |
|
| |
|
|
 |
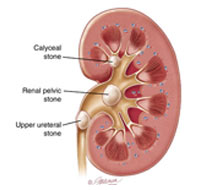
Endoscopic removal of urinary stones: PCNL, URS, RIRS, CLT |
|
|
Lithotripsy (ESWL) |
|
|
LASERS for stones and Prostate |
|
|
Monopolar and bipolar TURP |
|
|
HOLEP |
|
|
Urodynamics and uroflowmetry |
|
|
Laparoscopic urology surgeries |
|
|
Paediatric urology surgeries |
|
|
Urinary incontinence surgeries |
|
|
Surgeries for genitourinary cancers |
|
|
Reconstructive urology |
|
|
Microsurgeries for infertility and impotence |
|
| |
|
| |
 |
| |
|
| |
| |
| |
| |
| |
| |
| |
| |
| |
|